- Home
- About

- Animal Owners
- Membership
- Services
- Contact us

< Back
33rd Annual Scientific Meeting proceedings
Stream: LA
|
Session: Parallel Session: Standing surgery - (the classic), the new and the future
Date/Time: 07-07-2023 (09:00 - 09:30) | Location: Conference Hall Complex B
Date/Time: 07-07-2023 (09:00 - 09:30) | Location: Conference Hall Complex B
Standing Surgery of Recurrent Laryngeal Neuropathy
Rossignol F*1, Ducharme NG*2
1Grosbois Equine Clinic, Boissy Saint Leger, France, 2Cornell University Hospital for Animals, Ithaca, NY, USA.
Key Points
- The most important advantages of standing laryngoplasty is the ability to more accurately adjust the position of the arytenoid during the surgical procedure and avoidance of general anesthesia1.
- Standing laryngoplasty allows better exposure to the muscular process but proper restraints and head support are needed and there are technical differences in the surgical technique itself.
- The main technical aspect of the procedures are similar to laryngoplasty under general anesthesia.
- Selective laryngeal reinnervation can also be performed on the standing horse, allowing an improved access to the nerves and larynx
- For young horses that have never been raced and horses of high value because of their breeding potential, reinnervation can be offered because it is a more physiologically efficacious method of treating RLN.
The most relevant advantage of standing laryngoplasty and why we feel this should become the gold standard is that the degree of abduction can be adjusted far more accurately. Other advantages include avoidance of general anesthesia, better exposure of structures including muscular process, and rostral position of cranial esophagus: indeed, the dissection of the esophageal ostium from the muscular process is better performed with the patient standing. This is because coughing is heard during manipulation of the esophagus thus serving as a monitoring alarm during surgery. In addition, less force or tension on the sutures used to obtain abduction, can operate later in the day without as much concern for overtime pay by delayed recovery from general anesthesia. Finally, the procedure is easier to perform in the standing patient. The negative concerns would be less control of the patient and therefore of the sterile environment.
Patient Selection
When doing standing surgery under neuroleptanalgesia especially treating laryngeal hemiplegia, the first concern is the horse’s response to sedation. We performed laser ventriculocordectomy prior to the laryngoplasty, which allows better abduction during the Tie Back2. This helps identify horses which are “assertive” or “do not sedate well”. This is quite rare in our experience, especially in racing thoroughbred and professional owners’ sport horses
In our experience, laryngoplasty or revision laryngoplasty performed while the patient is standing allows for a better view and access to the cricoid cartilage and muscular process as compared to the recumbent laryngoplasties. It also allows to check the dissection of both the cricoid cartilage and muscular process under endoscopic guidance, and then to prevent any penetration of the laryngeal, pharyngeal and esophageal lumen. Furthermore, it allows more time to attempt to revise or improve a laryngoplasty by removing the concerns associated with general anesthesia.
In terms of difficulty, in our estimation standing laryngoplasty is easier to perform technically than recumbent laryngoplasty in race and sport horses
The standing surgery room should have a set of stocks that can be cleaned easily (preferably
stainless steel): the stock should allow easy access to the head and neck (the shoulders of the horse should rest near the front post). A head support should be present: details of an appropriate head support include allowing unencumbered access to the central larynx. It can be adjusted forward and backward depending on the horse and neck size and can be elevated or lowered easily. To protect hair contaminants, the clean horse is dressed with a “sleezy” with lateral opening for “left” or “right” side laryngoplasty (Fig 1). The halter is replaced by the head band without a throat latch strap. An ipsilateral eye cup to remove vision on the operating side is important. We think it is important that the contralateral eye is visual to keep the horse calm despite different degrees of sedation.
Anesthetic details
In a calm environment, proceed to the heart examination.
Then inject 0.02 mg/kg of Acepromazine (2 ml/500kg Calmivet) intravenousely, 10-15 minutes before taking the horse from the stall. Just before putting the horse in the stock, inject intravenously detomidine 0.01mg/kg and Morphine 0.1 mg/kg
For laser ventriculocordectomy, instile 20 ml of Bupivacaïne and 100 ml of Lidocaine in pharyngo-laryngeal cavity and nasal cavities.
For standing laryngoplasty or nerve graft, plug in the catheter Romifidine syringe (Sedivet ND) and administrate 0.5 ml to start and follow with 0.01mg/kg around every 10 minutes. Usually, we carry on administrating 0.01mg/kg Romifidine (0.2-0,3 mL/ 500 kg de Sedivet ND) around every 3-5 minutes to keep the horse in adequate sedation but this is highly variable. A CRI can also be used.
The endoscope is then placed near the tip of the epiglottis (local anesthesia is also applied to the larynx and the endoscope secured to the nose band with a Velcro band (TURN OFF THE ENDOSCOPE LIGHT). After aseptic preparation of the surgical site and prior to application of local infiltration of anesthesia, the ventral aspect of the linguofacial vein is marked with 2-3 staples. Lidocaine (10 to 15 ml) is infiltrated up to the incision using an inverted U-shaped line. Draping is performed with independent “edge” adherent drapes and a custom-made drape with a rectangular limited opening.
Standing Laryngoplasty
Standard incision ventral to the linguofacial vein. Because of gravity, the vein is a little more ventral than during recumbency: identify the ventral border of the linguofacial vein in the middle of the incision then extend the incision caudally and cranially. The collateral blood vessels and innervation comes from the caudal aspect of the incision: be prepared with readily available local anesthesia if needed. The access to the cricoid and muscular process varies with head flexion and this is variable between horses which have cervical and cephalic positions of their larynx: marked head extension is positive during recumbent laryngoplasty but is a negative during standing laryngoplasty. The cricopharyngeus muscle is not desensitized with C2-C3 block nor with perilaryngeal application of local anesthesia and must often be infiltrated with local anesthesia. A caudal approach, by approaching the CAD muscle and MP caudal to the cricopharyngeus muscle, has replaced the initial lateral approach. It reduces the dissection and the risk of injury of the cranial laryngeal nerve. Always identify the cranial esophagus over muscular process. After the sutures are placed, the degree of abduction is monitored (Fig 2) and adjustments are made as needed. Routine closure is performed.
Technique is similar to laryngoplasty performed on general anaesthesia. The technique is continuously refined. The author is using metallic implants both at the MP and cricoid cartilage to reinforce the laryngoplasty construct and prevent tearing of the cartilages (Fig 3)
Standing nerve graft
A more physiologically viable treatment option for Recurrent Laryngeal Neuropathy (RLN) involves reinnervation of the cricoarytenoid dorsalis muscle (CAD). The omohyoideus muscle is innervated by a nerve formed by the first and second cervical nerve branches, hereafter referred to as the C1/C2 nerve. These nerves can be transplanted to the CAD. The nerve-implantation technique is replacing the nerve-pedicle procedure3.
Although any horse with RLN is a candidate for laryngeal reinnervation, younger horses and those with grade 3 laryngeal movements are the ideal candidates for this surgical procedure. Sport horses with grade 3 RLN are also excellent patients for reinnervation, as these horses have a long career. Such physiological procedures should provide optimal long-term functional results while preventing complications such as coughing. The procedure was initially performed under general anesthesia but is now performed in the standing patient in almost all cases
Patient preparation, positioning, anesthetic protocole and the initial surgical approach are similar to laryngoplasty. The caudal approach offers improved access to the CAD, does not involve any myotomy of the cricopharyngeus muscle, and reduces the risk of post-operative constriction of the nerve by scar tissue. The selected main branch of the nerve is implanted through a tunnel using a Reverdin needle from medial to lateral and secured to the lateral or medial belly of the CAD muscle. Any excess nerve branch is implanted directly in a small slit in the medial muscle belly of the CAD as described (Fig 4).
Since January 2019, we are using the ventral branch the Spinal Accessory Nerve (SAN), or XI cranial nerve, for laryngeal selective reinnervation. This is a large motor nerve, located at the caudal aspect of the larynx. Its dorsal branch innervates the brachiocephalicus and trapezius muscle, and its ventral branch innervates the sternocephalicus (or sternomandibularis) muscle. The function of the latter includes flexion and rotation of the neck. We performed an EMG study and showed that the sternomandibularis muscle is strongly activated at galop during inspiration4. It seems to be an ideal nerve for equine laryngeal selective reinnervation. It can be grafted in associated with C1-C2 or alone. Usually, the SAN is grafted into the lateral belly and C1-C2 into the medial belly of the CAD. Specific indications and technique will be discussed.
Standing Dynamic Neuro Prothesis (DNP): emerging treatment
This is a concept of enhanced nerve graft based on the observations 1) that some horses with more advanced RLN take a longer time to rehabilitate and 2) that some horses with less severe RLN and having undergone tie-back surgery show an abduction level at exercise beyond the resting tieback level. Therefore, in a subpopulation of RLN horses, DNP may be indicated in cases of laryngeal reinnervation in which a more advanced degree of muscular atrophy of the CAD is present, requiring a longer period of muscle rehabilitation. The goal of the DNP is 1) to reduce the rehabilitation period currently needed to allow time for reinnervation and 2) to improve the effect of reinnervation on the degree of abduction. The principle of the technique is to place a modified laryngoplasty suture over the separation of the medial and lateral compartment of the CAD muscle and add nerve implants. The suture stabilizes the arytenoid in a neutral position, that is sufficient to reduce the driving airway pressure during inhalation and make it very likely that stimulations of the transplanted nerves (+/- native nerve) will be strong enough to increase the airway diameter at exercise. This technique also enables to reduce fatigue of the re-animated CAD and prevent associated midline collapse of the arytenoid cartilage. Up to this day, 130 horses have been operated with promising results. Objective data needs to be collected before drawing conclusions about this new concept.
Figures

Fig 1: Preparation of the horse for standing tieback or nerve graft. Note the head support that can be adjusted forward and backward depending on the horse and neck size and can be elevated or lowered easily. To protect hair contaminants, the clean horse is dressed with a “sleezy” with lateral opening for “left” or “right” side laryngoplasty. An ipsilateral eye cup is placed to remove vision on the operating side.

Fig 2: Per-operative endoscopic images of a larynx during a tieback. Assessment of the arytenoid position under GA (left) or on the standing horse (right)
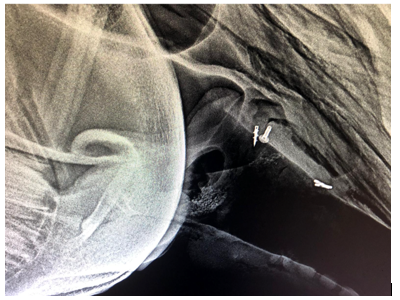
Fig 3: Use of metallic implants at the MP (Titanium screw and titanium 3D printed sleeve) and at the cricoid cartilage (Titanium suture buttons) to reinforce the laryngoplasty suture.
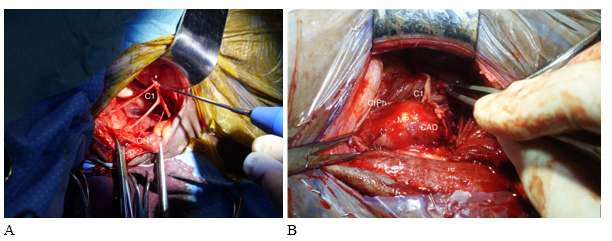
Fig 4A: Isolation of the C1-C2 nerve branches is facilitated by easy ventral mobilization of the OH. C1: C1-C2 nerve branches; OH: Omohyoideus muscle
Fig 4B: C1-C2 nerve branches could be observed free of tension implanted in the CAD just caudal to the CrPh muscle. MP: Muscular process. CrPh: cricopharyngeus muscle retracted rostrally
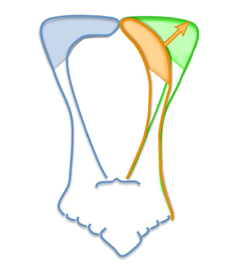
Fig 5: Concept of hybrid procedure of DNP: Partial abduction of the left arytenoid cartilage is provided by a modified laryngoplasty (orange). Increased airway diameter provided by stimulations of the transplanted nerves +/- native nerve (green)
References
- Rossignol Rossignol F, Vitte A, Boening J, et al. Laryngoplasty in standing horses. Vet Surg 2014; 44:341-347.
- Perkins JD, Meighan H, Windley Z, et al: In vitro effect of ventriculocordectomy before laryngoplasty on abduction of the equine arytenoid cartilage. Vet Surg 2011; 40:305-310.
- Rossignol F, Brandeberger O, Perkins JD et coll. Modified nerve transplantation technique for treatment of recurrent laryngeal neuropathy in horses by tunnelling the first or second cervical nerve through the crico-arytenoideus dorsalis muscle. Equine Vet J. 2018; 50(4):457-464.
- Campos Schweitzer A, Mespoulhès-Rivière C, Möller D et al : Laryngeal reinnervation using the spinal accessory nerve: Electromyographic study of the sternomandibularis muscle. Equine Vet J. 2023; 55(3):515-523.
This website uses cookies to improve your experience and for traffic analysis. If you continue, we’ll assume that you agree to the use of cookies as stated in our Cookie Policy.